Berikut kutipan ilmiah kedokteran yang sangat bermanfaat bagi Penulis sehingga disusun dan digunakan sebagai referensi pribadi.
Perpustakaan Keluarga : Helmut Todo Tua Simamora dan dr. Olga Y.V Hutapea
Doctors may be performing too many repeat colonoscopies on people who've had pre-cancerous polyps removed during an earlier colon cancer screening, a new Norwegian study suggests.
Many of these patients have no greater risk of dying from colon cancerthan the general public, the researchers determined.
People who have a single low-risk polyp removed have a much lower risk of colon cancer, compared to both the general public and patients who have multiple polyps or aggressive polyps removed, said lead author Dr. Magnus Loberg, a lecturer in health management and health economics at the University of Oslo.
These low-risk patients likely don't need the aggressive follow-up called for under current guidelines, Loberg said.
"These findings support more intense surveillance of the high-risk group, but should maybe lead to reconsideration of the guidelines regarding the low-risk group," he said. The study is published in the Aug. 28 issue of the New England Journal of Medicine.
Current guidelines recommended by the American Cancer Society call for repeat colonoscopy at 5 to 10 years for patients who have one or two small, non-aggressive polyps removed, based on risk factors such as family history and prior health problems. People with large or aggressive polyps are encouraged to receive repeat colonoscopy every 3 years.
About one-quarter of all colonoscopies performed in the United States are done as increased cancer surveillance for patients who had polyps removed during earlier colonoscopies, said Dr. David Lieberman, chief of gastroenterology at Oregon Health and Science University in Portland, Ore.
"That's a lot of colonoscopy, and if we don't need to do as many, that potentially would free up more resources and enable more screening exams to be done on new patients," Lieberman said.
"These data would suggest a 10-year follow-up would be fine for most patients with low-risk polyps," he added.
The study involved nearly 41,000 patients in Norway who had colorectal polyps removed during a colonoscopy between 1993 and 2007.
Researchers sorted the patients as low-risk or high-risk based on the size of the removed polyp, and whether they had more than one polyp removed. They then tracked how many died from colon cancer through 2011.
Patients in Norway who had a single polyp smaller than 1 centimeter removed during an earlier colonoscopy had a 25 percent reduced chance of death from colon cancer, compared to the general population, researchers found.
At the same time, patients who had multiple polyps or larger polyps removed ran a 16 percent increased risk of colon cancer death.
"As expected, the high-risk group had increased risk of colorectal cancer death compared with the general population, while the low-risk group had a stronger risk reduction," Loberg said. "This really questions the recommendations that are given now" for low-risk patients.
Lieberman noted that since the study took place in Norway, it might not correspond perfectly to America.
For example, Norway had no colon screening program set up during the study period, so the people who underwent colonoscopy likely had symptoms that led doctors to suspect some sort of health problem.
Also, Norway is less ethnically diverse than the United States, which could make a difference, he said.
"It would be important to try to get this kind of information in the United States, to better inform our screening policies," said Lieberman, who wrote an editorial accompanying the study.
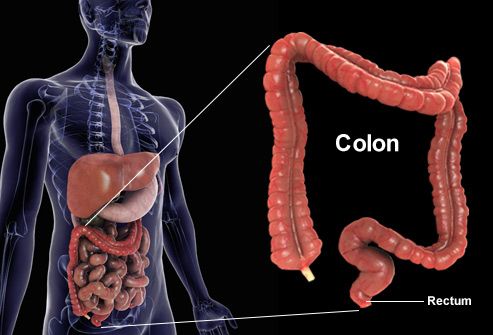
Colorectal Cancer: What Is It?
Not including skin cancer, colorectal cancer is the third most frequently diagnosed cancer in men and women and the second highest cause of cancer deaths in the U.S. Yet, when found early, it is highly curable. This type of cancer occurs when abnormal cells grow in the lining of the large intestine (colon) or rectum. Learn more about who gets colorectal cancer, how it is detected, and what the latest treatments can accomplish.
Colorectal Cancer: How It Starts
Colorectal cancers often begin as polyps -- benign growths on the interior surface of the colon. The two most common types of intestinal polyps are adenomas and hyperplastic polyps. They develop when there are errors in the way cells grow and repair the lining of the colon. Most polyps remain benign, but some have the potential to turn cancerous. Removing them early prevents colorectal cancer.
Risk Factors You Can't Control
Your risk of colorectal cancer depends on genetics and lifestyle. Factors you can't control include:
- Age -- most patients are older than 50
- Polyps or inflammatory bowel disease
- Family history of colorectal cancer
- History of ovarian or breast cancer
Risk Factors You Can Control
Some factors that raise the risk of colorectal cancer are within your control:
- Diet high in red or processed meats, or meats cooked at high temperatures
- Being obese (excess fat around the waist)
- Exercising too little
- Smoking or heavy alcohol use
Colorectal Cancer Warning Signs
There are usually no early warning signs for colorectal cancer. For this reason it's important to get screened. Detecting cancer early means it's more curable. As the disease progresses, patients may notice blood in the stool, abdominal pain, a change in bowel habits (such as constipation or diarrhea), unexplained weight loss, or fatigue. By the time these symptoms appear, tumors tend to be larger and more difficult to treat.

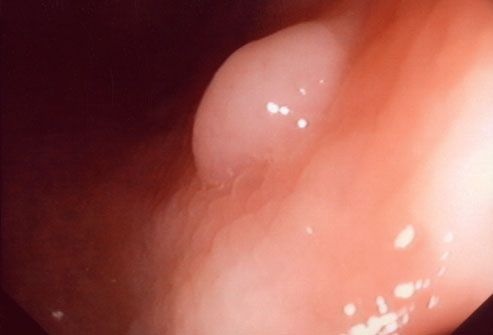
Colorectal Cancer Screening
Because colorectal cancer is stealthy, screenings are the key to early detection. Beginning at age 50, most people should have a colonoscopy every 10 years. This procedure uses a tiny camera to examine the entire colon and rectum. These tests not only find tumors early, but can actually prevent colorectal cancer by removing polyps (shown here).
Virtual Colonoscopy
There is now an alternative to colonoscopy that uses CT scan images to construct a 3-D model of your colon. Called virtual colonoscopy, the procedure can reveal polyps or other abnormalities without actually inserting a camera inside your body. The main disadvantage is that if polyps are found, a real colonoscopy will still be needed to remove and evaluate them.
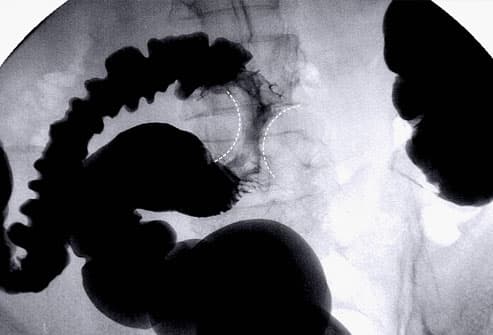
X-Rays of the Colon (Lower GI)
X-Rays of the colon -- using a chalky liquid known as barium as a contrast agent -- allow your doctor a glimpse at the interior of the colon and rectum, offering another way to detect polyps, tumors, and changes in the intestinal tissue. Shown here is an "apple core" tumor constricting the colon. Like the virtual colonoscopy, any abnormalities that appear on the X-rays will need to be followed up with a conventional colonoscopy.
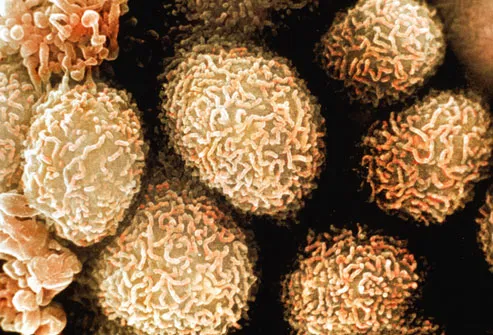
Diagnosing Colorectal Cancer
If testing reveals a possible tumor, the next step is a biopsy. During a colonoscopy, your doctor will remove polyps and take tissue samples from any parts of the colon that look unusual. This tissue is examined under a microscope to determine whether or not it is cancerous. Shown here is a color-enhanced, magnified view of colon cancer cells.
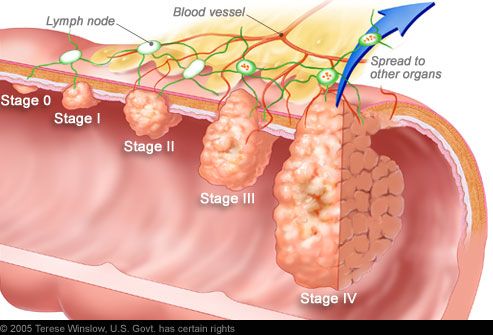
Staging Colorectal Cancer
If cancer is detected, it will be "staged," a process of finding out how far the cancer has spread. Tumor size may not correlate with the stage of cancer. Staging also enables your doctor to determine what type of treatment you will receive.
- Stage 0 -- Cancer is only in the innermost lining of the colon or rectum.
Colorectal Cancer Survival Rates
The outlook for your recovery depends on the stage of your cancer, with higher stages meaning more serious cancer. The five-year survival rate refers to the percentage of people who live five years or more after being diagnosed. Stage I has a 74% five-year survival rate while stage IV has a five-year survival rate of only 6%.
Colorectal Cancer Surgery
In all but the last stage of colorectal cancer, the usual treatment is surgery to remove the tumor and surrounding tissue. In the case of larger tumors, it may be necessary to take out an entire section of the colon and/or rectum. The good news is that surgery has a very high cure rate in the early stages. If the cancer has spread to the liver, lungs, or other organs, surgery is not likely to offer a cure -- but removing the additional tumors, when possible, may reduce symptoms.
Treating Advanced Colorectal Cancer
When colorectal cancer has spread to one or more lymph nodes (stage III), it can still sometimes be cured. Treatment typically involves a combination of surgery, radiation (being administered here), and chemotherapy. If the cancer comes back after initial treatment or spreads to other organs, it becomes much more difficult to cure. But radiation and chemotherapy may still relieve symptoms and help patients live longer.
Coping With Chemotherapy
Chemotherapy has come a long way from the days of turning people's stomachs. Newer drugs are less likely to cause this problem, and there are also medications to control nausea if it does occur. Clinical trials continue to search for chemotherapy drugs that are more effective and tolerable.
Radiofrequency Ablation
Radiofrequency ablation (RFA) uses intense heat to burn away tumors. Guided by a CT scan, a doctor inserts a needle-like device that delivers heat directly to a tumor and the surrounding area. This offers an alternative for destroying tumors that cannot be surgically removed. In patients with a limited number of liver metastases that cannot be removed by surgery, chemotherapy is sometimes combined with RFA for tumor destruction.
Preventing Colorectal Cancer: Diet
There are steps you can take to dramatically reduce your odds of developing colorectal cancer. Researchers estimate that eating a nutritious diet, getting enough exercise, and controlling body fat could prevent 45% of colorectal cancers. The American Cancer Society recommends a diet that emphasizes fruits and vegetables, helps you keep a healthy weight, limits processed and red meat, and includes whole grains instead of refined grains.
Preventing Cancer With Exercise
Physical activity appears to be a powerful weapon in the defense against colorectal cancer. In one study, the most active participants were 24% less likely to have the cancer than the least active people. It didn't matter whether the activity was linked to work or play. The American Cancer Society recommends exercising five or more days a week for at least 30 minutes a day. Vigorous exercise gives you even more benefits in less time -- 20 minutes 3 or 4 days a week.
Sumber :MD
Tidak ada komentar:
Posting Komentar